

The menisci are very important structures that protect the articular cartilage of the knee from excessive wear. Any suspicion of a meniscal injury should be carefully diagnosed, and if any damage is found, appropriate treatment should be implemented. There are many types of meniscal injuries - some of them (e.g. small tears, bruises) can be treated conservatively, while others require surgery. A particularly disadvantageous situation is when the damaged part of the meniscus is unstable and begins to damage the cartilage surface of the knee joint, as this can lead to its destruction and rapid degeneration of the knee.
Make an appointment now - to see a doctor specializing in arthroscopic meniscal suturing at our hospital
[title]
[image-intro]
[readmore text="Read more"]{/article}
[title]
[image-intro]
[readmore text="Read more"]{/article}
[title]
[image-intro]
[readmore text="Read more"]{/article}
One of the treatment options is arthroscopic suturing of the damaged meniscus. The advantage of this method is the preservation of its own natural meniscus, which initially fits perfectly to the shape of the articular surfaces, thus preserving the biomechanics of the joint and the protective function of the meniscus. Knee arthroscopy enables both the precise assessment of a meniscus injury and the simultaneous undertaking of repair procedures. The arthroscopic meniscus suturing procedure is performed without the need to open the joint - the surgeon makes small incisions (approx. 8 mm) through which he introduces a camera and miniature tools, and the inside of the knee is monitored during the procedure on the monitor.
The knee meniscus function
There are two menisci in the knee: medial and lateral. The role of the knee meniscus is to:
shock absorption when transferring body weight to the limb,
transferring the compressive forces more to the circumference, thanks to which the cartilage of the central knee joint is subjected to less stress - when the knee is straightened, the menisci transfer 50% of the compressive force, and when the knee is bent to 90 degrees, menisci can carry up to 85% of the load [1];
optimal complement to the anatomically mismatched surface of the femur and tibia. Partial or complete removal of the meniscus (meniscectomy) increases the point pressure on the articular surfaces and the subchondral bone and reduces the stability of the knee, which leads to faster development of joint degeneration;
precise distribution of synovial fluid;
proprioceptive function - activating quick neuromuscular reflexes that have a protective function for the joint by quickly releasing muscle tension, preventing uncontrolled movement in the joint;
increasing the stability of the joint throughout the range of motion.
Symptoms of meniscal damage
A meniscus rupture can occur as a result of acute trauma or as a result of aggregation of microdamages - for example, degenerative changes, incorrect axis of the lower limb, etc. Acute meniscal damage is most often the result of uncontrolled rotation of the shin with the bent and stressed knee. The outward twist of the shin predisposes to rupture of the medial meniscus, while the inward rotation of the lateral meniscus. As the medial meniscus is less mobile, a greater percentage of injuries are injuries to the medial meniscus, especially its posterior horn.
In the event of a severe trauma, a rupture of the meniscus may be one of the elements of a knee injury, e.g. very common damage to the medial meniscus and tibial collateral ligament and rupture of the anterior cruciate ligament (ACL) occurs very often. A knee injury is then called the O'Doneghue triad and usually occurs as a result of a strong impact to the lateral side of the bent knee joint during a game of football or basketball or skiing.
In the case of acute meniscal damage with a displacement of its fragment, a click may be heard in the knee joint, accompanied by sudden pain and sometimes blockage of movement in the joint. Attempting to extend the blocked knee causes the symptoms to intensify. Swelling may occur within hours, especially if there is simultaneous damage to the cruciate and / or medial collateral ligaments. You may not be able to put pressure on your knee because of the severe pain. Such a situation always requires urgent knee arthroscopy preceded by a knee resonance imaging (MRI).
Degenerative meniscal damage may be a local rupture or delamination of the meniscus and may not be so symptomatic. Degenerative meniscal damage may not be painful at all, may be symptomatic periodically and even spontaneously resolve. Most often they have the form of an oblique horizontal stable fracture in the posterior corner of the medial meniscus. It is important to be aware that cracks will never heal by themselves, they will always progress slowly - spreading over more and more of the meniscus. They are also always associated with a greater risk of tearing off a fragment of the meniscus and producing more damage to the joint, making the damage to the meniscus irreparable. This can happen even during normal activities, such as getting up from a crouching position. Chronic pain is an indirect indication of cartilage damage and requires consideration of arthroscopic treatment of the meniscus.
The risk of meniscus damage is greatest in people:
with incorrect positioning of the lower limb - valgus of the knees overloads the lateral meniscus, and varus in the knees overloads the medial meniscus,
with knee instability, most often due to damage to the anterior cruciate ligament ACL,
practicing contact sports and other dynamic sports, with poor neuromuscular control of the knee,
overweight.
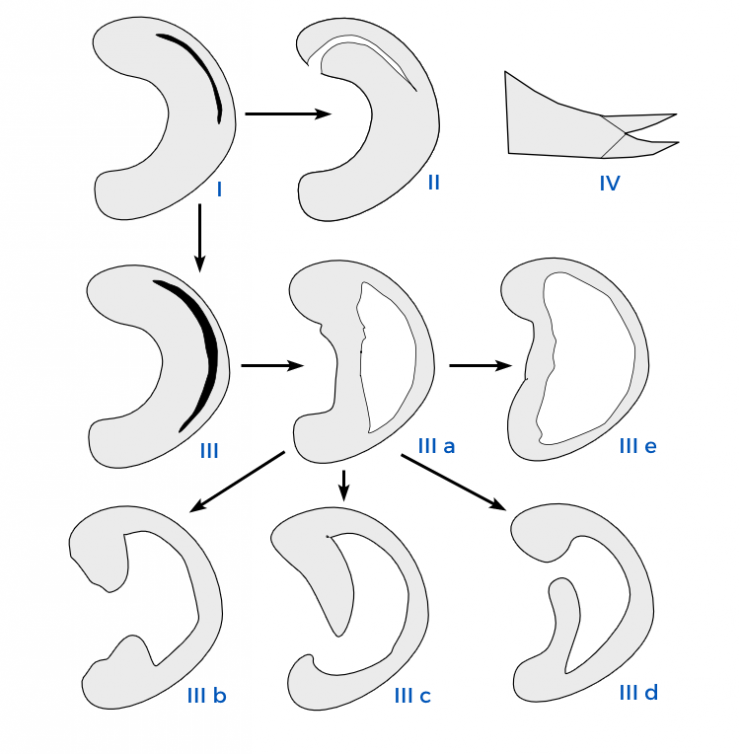
Types of meniscal tears
Depending on the course of the meniscal tear line, the following types of meniscus damage are distinguished:
longitudinal vertical (e.g. bucket handle),
transverse (radial),
horizontal (delamination),
oblique, e.g. of the "parrot's beak" type,
folded.
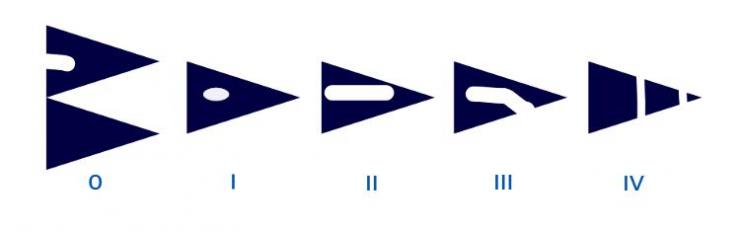
Another, equally important division of meniscal tears is based on the morphology of the fracture in the cross-section of the meniscus as visualized in the knee MRI. Simply put, degree I and II injuries do not qualify for surgical treatment, and third and fourth degree injuries should be operated on.
Depending on the severity of the meniscus rupture in the magnetic resonance imaging, we distinguish 4 types of damage:
internal damage, very common. We treat non-surgically only in the case of clear pain.
more extensive internal damage - the same procedure as for type I.
lesions exceeding the articular surface of the meniscus - most often symptomatic, but not showing signs of blocking the joint or jumping. If they are left unoperated, the damage may increase, damage to the cartilage and transform to type IV.
require urgent surgical treatment - knee arthroscopy with an attempt to stitch and repair. It is much easier to suture the meniscus in the third degree of damage than in the fourth one.
The healing potential of the meniscus largely depends on the degree of perfusion in the damaged area. In children, the menisci are supplied by blood vessels along almost their entire width. With age, the depth at which the blood vessels reach decreases - in an adult it is only 1/3 of the circumferential part of the meniscus, approx. 6 mm wide In this peripheral zone (the so-called "red"), the meniscus may heal spontaneously with adequate early diagnosis and rehabilitation.
Eligibility for meniscal suturing surgery
Surgical treatment consisting in suturing the meniscus is considered taking into account the following factors:
the shape of the meniscus damage - vertical injuries with a straight line of a meniscus rupture (knee MRI) heal best,
localization of meniscal damage - the closer to the vascularized part of the meniscus the damage is, the greater the chance of full healing while maintaining the consistency and function of the meniscus,
the time that has elapsed since the meniscus injury - fresh traumatic injuries of the meniscus are better healed (up to 6-8 weeks) than the worsening damage resulting from many years of meniscal degeneration (interview)
patient's age - meniscus suturing procedures performed in people up to 40 years of age are the best prognosis (interview),
knee stability, presence of other accompanying injuries (examination),
correct knee axis (examination),
neuromuscular coordination, knee muscular capacity (test).
In qualifying for surgery, the symptoms reported by the patient (severe pain and blocking the knee) and the confirmation of the meniscus injury by magnetic resonance imaging are important. In some cases, it is possible to determine before the planned surgery whether a damaged meniscus will tend to repair and continue to perform its function after suturing. There are also situations where only during arthroscopy it turns out that suturing the meniscus will not be possible to a satisfactory degree and that part of the meniscus will have to be removed.
Suturing a damaged meniscus
Knee arthroscopy begins with a careful assessment of damage to the meniscus and other knee structures. Then, the optimal technique of suturing the meniscus is selected, depending on the location of the damage, the surgeon's preferences, the availability of additional implants and specialized instruments dedicated to suturing the meniscus.
There are many different techniques of suturing the meniscus, methods of reaching the site of damage, opinions on whether to sew the meniscus with absorbable sutures or not, or use special implants - the so-called staples, anchors or better not.
Each suturing of the meniscus is an individual procedure that requires various variable decisions during the procedure. The more experienced the orthopedist and the better equipped the operating theater, the more flexible and optimally the meniscus repair procedure can be performed. Sewing must take into account the zone in which sewing is performed, because depending on it, you need to sew seams in a different direction. Sewing must be a compromise between a strong and stable fixation (e.g. non-absorbable sutures, staples) and biology, during which the meniscus can remodel itself to the articular surface during reconstruction, so that it again fits perfectly with the cartilage in the joint. Particularly difficult treatments are repositions of completely detached meniscus - the so-called type of bucket handle.
If there is simultaneous traumatic injury to the anterior cruciate ligament of the knee, suturing the meniscus and reconstructing the knee should be performed during one arthroscopy.
Below is a video from the arthroscopy of one of our patients (operator Grzegorz Jarosławski) - the entire procedure was performed with the use of absorbable threads.
Contrary to sewing the meniscus with ready-made anchors made of polystyrene threads and PEEK (polyether ether ketone) anchors, using our sewing method, after 8 weeks there are no suture residues in the knee.
Rehabilitation after arthroscopic suturing of the meniscus
After the meniscus suturing procedure, the operator individually determines the basic rules of conduct for the next 6 weeks. They concern the allowable range of knee motion, the possibility of weighting, the necessity to use elbow crutches or an orthosis.
Excessively early bending of the knee or performing rotational movements may damage the sutures and cause the meniscus repair site to tear. In order to reduce post-operative knee swelling and post-operative pain at the hospital, the Game Ready device is used at the Dworska Hospital, which is based on optimal compression and cooling of the operated joint.
It is important to start recreating a symmetrical physiological gait as early as possible, so that no abnormal patterns are generated, as is the case with walking by 1 elbow ball with only one limb loaded.
The patient leaves the hospital within the first day after the arthroscopic procedure with recommendations to be carried out at home for the next few days:
lifting the operated leg above the hip level,
exercises of the range of motion of the ankle joint,
applying cool compresses on the knee - 15 minutes every 2 hours,
quadriceps isometric exercises.
Rehabilitation after suturing the meniscus should be continued under the supervision of an experienced physiotherapist for about 3 months. The range of motion and the percentage of loading on the operated leg are gradually increased after consultation with the orthopedist and on condition that the patient does not experience any pain. Exercises after suturing the meniscus should take into account the correct activation of the muscles stabilizing the knee joint, because once damaged meniscus, even after healing, will not be as durable as before the injury. Proper muscle strengthening can protect the meniscus from overstrain and reduce the risk of recurrence. Return to normal full activity is possible in 3-4 months after the procedure.
Rehabilitation after ACL reconstruction and suturing of the meniscus (when both procedures were performed as part of one procedure) requires even more skilful balancing of the introduction of flexion and compression at the appropriate stage of rehabilitation. If the reconstruction of the ACL ligament was performed with an own graft, the period between 8 and 12 weeks is characterized by a decrease in the strength of the graft and an increased risk of its rupture. Return to normal daily activity in the case of simultaneous suturing of the meniscus and ACL reconstruction is prolonged and may occur 3 - 6 months after the procedure. Return to sport is possible between 8 and 12 months depending on the progress of rehabilitation and the type of sport practiced.
Other treatments for meniscal tears
Not all types of meniscal tears are surgically treated. In the case of small, stable tears of the meniscus up to 10 mm, conservative treatment is attempted with skilfully conducted rehabilitation.
Not all meniscal injuries qualified for surgery can be repaired by suturing. Tears in the non-bleeding part, extensive destruction or aged meniscus injuries must be treated by removing all or part of the meniscus (meniscectomy). In this case, a transplant can be performed that will replace the function of the natural meniscus. Depending on the degree of damage to the meniscus, the procedure can be performed:
implantation of the entire meniscus taken from a tissue bank (allograft),
implantation of a fragment of a synthetic meniscus (with the roots of the meniscus preserved) - made of polyurethane or collagen (Menaflex or Actifit).
Sources:
[1] Uszkodzenia kolana [w:] Brotzman S.B, Wilk K.E.: „Rehabilitacja ortopedyczna” tom 2, Elsevier Urban & Partner 2008, s. 481-488.
Important information
| Duration of the procedure (depending on the method) | 30 - 120 minutes |
| Basic tests required for the procedure | basic - preparation for surgery tab |
| Anesthesia | subarachnoid |
| Hospital stay | 4 - 8 hours |
| The period of significant dysfunction - walking on crutches with relief of the limb | up to 2 weeks |
| The period of limited dysfunction - walking with the protection of elbow crutches | 3 - 6 weeks |
|
Removal of stitches |
12 - 16 days |
| Change of dressings | every 3-4 days |
| Contraindications to the procedure | overweight, infection, knee axis disorders |
Frequently asked questions about arthroscopic suturing of the meniscus
A typical symptom at the moment of acute meniscal damage with a fragment of its fragment torn off is a perceptible crunch or audible click in the knee, severe pain and joint blockage (most often in flexion). Trying to move your knee aggravates the pain. It may be difficult or impossible to stand on the injured leg. In minor injuries of the meniscus, the symptoms are less intense - the pain may appear only during activities that put a lot of strain on the knee (running, jumping), and the feeling of jumping in the knee may be temporary and the patient is able to unblock them by means of manipulations known to him.
Relieving the knee is designed to heal the stitched meniscus. The time of walking on crutches depends on the site, extent and nature of the meniscal damage and is usually 6-8 weeks. During this period, the percentage of weight bearing on the knee is gradually increased after consultation with the orthopedist and provided that it does not cause pain in the patient.
Exercises for the knee after suturing the meniscus should be carried out under the supervision of an experienced physiotherapist who will plan the therapy process and teach exercises that will be safe for the operated meniscus (they will not disturb the healing process). proper activation of the muscles responsible for the stability of the joint and improvement of the strength and endurance of the muscles of the lower limb. The ultimate goal of the exercises is to protect the operated meniscus from excessive strain due to proper control of the knee movements both during daily activities and during sports activities.




